In our regular series, Dr Martin Vernon, our clinical lead for frailty and consultant geriatrician at Tameside and Glossop Integrated Care NHS Foundation Trust, answers questions about the Covid-19 pandemic.
Q: When did you first become aware of Covid-19?
A: Although the disease was not officially named until mid-February 2020, I became aware in late January via news and social media channels of a SARS-like viral illness in China and that other cases were being reported in neighbouring countries. By the end of January 2020 I was already aware that the World Health Organisation had declared a global health emergency caused by this illness.
Q: Do you remember when you first realised this would be the first worldwide pandemic in over 100 years and change your working life for months?
A: As soon as the news emerged of two cases in the UK testing positive for coronavirus at the end of January 2020 it seemed highly likely that the virus would spread quickly around the world as a result of air travel.
This was reinforced by the widely reported decision of US authorities in late January 2020 to close its borders to any foreign nationals travelling to China in the preceding 14 days. Following large numbers of reported deaths and cases in China in the first week of February 2020 and the official naming of Covid-19 there were then multiple reports of outbreaks hitting the media which made it clear that we were heading into a pandemic that would affect us all for a long time ahead.
For me the turning point came with the widely reported surge in cases in Italy at the end of February 2020. The lockdown in Lombardy together with emerging stories of Italian hospital oxygen supplies under pressure and outbreaks in care homes led to a quick realisation that the UK would also be in lockdown soon, with the NHS likely to be under the same pressure being experienced by colleagues in mainland Europe.
Q: What has been the most challenging aspect of working in your area during Covid-19?
A: I moved jobs at the end of January 2020, simultaneously taking up a clinical role in a new hospital and moving from a national leadership role to more regionally focused leadership roles in both London and Greater Manchester.
Not only did I have to rapidly decide where to optimally deploy myself clinically, but also, I quickly realised that travelling around the country to undertake other roles was out of the question. This meant quickly getting to know new teams, a new clinical environment and its systems, establishing new service offers and adopting new ways of remote working.
All of this was extremely challenging from the outset. Yet despite this, there rapidly emerged a sense of shared purpose and liberation promoted through remote and digital working. This helped to quickly break down barriers and promote effective team working in ways that I had never previously experienced in over 30 years of providing healthcare.
Q: Has there been a low point during the pandemic professionally and if so, what was it and how did you overcome it?
A: In late March and early April 2020 I realised that national policy decisions appeared to have left care homes, their residents and care staff largely unprotected from the impact of the pandemic.
Elsewhere in Europe we had already seen the catastrophic impact of Covid-19 on older people in care homes. Along with colleagues with whom I conferred locally, nationally and internationally, I felt growing alarm that more had to be done if we were to avoid the same catastrophe in England.
Witnessing care home outbreaks with high mortality across the country was a particular low point, subsequently revisited many times over as ONS data emerged confirming considerable excess care home mortality in England.
Despite this, I was fortunate to work with academic, clinical and industry colleagues in Greater Manchester and nationally to quickly do all we could to develop and deploy digital tools and use the resources available to help care homes deal with the pandemic in real time. On my own patch, working with colleagues in the local authority, CCG, public health, primary and secondary care, we were able to develop and test effective new ways of detecting and responding proactively to clinical deterioration among care home residents.
This helped identify outbreaks early and optimise public health responses to better support and protect residents and staff. The learning derived from this work has been recurrently shared across Greater Manchester clinical networks and with colleagues around the country.
Alongside multidisciplinary leaders nationally, I was also privileged to help successfully lobby Government to shift policy towards implementing systematic care home testing and bring greater scrutiny through research on the impacts and opportunities presented by the pandemic to do more to enhance care for care home residents.
Q: Are there any positives you can take from the pandemic professionally?
I have been particularly struck by the commitment, professionalism and team spirit shared by colleagues across all parts of the health and care system.
While facing the biggest challenge of our careers, everyone deployed in the public sector has gone well above and beyond the call of duty.
Despite us all experiencing overwhelming work and professional demands, tiredness and at times personal and professional tragedy, we have kept going.
The country is incredibly fortunate to have a dedicated workforce with such widespread compassion and dedication to preserving the health, safety and dignity of the people for whom they provide care, regardless of how and where they live.
|
The Network is supporting the further roll out of the ‘EARLY’ identification tool - a new electronic search device which supports shared decision making and having well-planned, coordinated care.
The tool has been developed in the North West and piloted across primary care in the region, as well as in London. It is responsive to a person’s changing needs, with the aim of always improving the experience of care.
The Network will be expanding on the successful pilot and supporting further roll out of the EARLY identification tool in primary care, with a package of support from a GP Facilitator.
If people can be identified early enough it will provide the opportunity to engage in planning with people, through a personalised care conversation, enabling people to explore their wishes and preferences for their care both now and in the future.
As part of the EARLY process, conversations can be recorded and with consent shared on a local Electronic Palliative Care Coordination System (EPaCCS). The EARLY process supports the system in working towards personalised care and crucially it increases the choice and control people receiving palliative care have over their lives.
If you would like further information of how to get involved please contact England.GMEC-EOLC@nhs.netbefore Friday, August 20, 2021.
More information can be found on the EARLY identification tool here.
The Network is aiming to boost the promotion of two major diabetes programmes following the appointment of three engagement officers.
The new recruits will provide GP surgeries with tailored support to help increase the take-up rate to the “Healthier You” Diabetes Prevention Programme and to support GP Surgeries with completing online registrations for Diabetes My Way.
Here are the three new recruits:
  There is still one vacancy available. If you would like to find out more information please contact Rebecca.murray@xylahealth.com
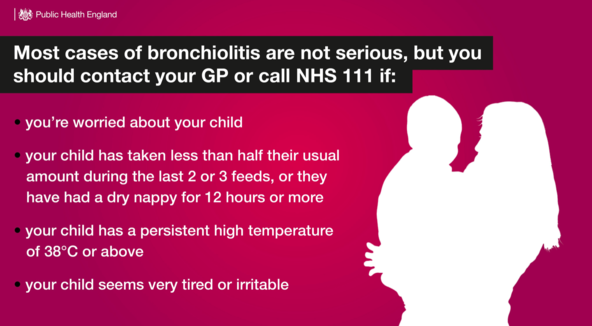
The Children and Young People Network has been working with clinicians, provider organisations and commissioners across the system to plan for an expected early winter surge of Respiratory Syncytial Virus (RSV).
The virus is among other respiratory causes of bronchiolitis which can make small babies, as well as children usually under two years old, quite poorly.
Although only a small percentage of babies will require hospital care, this year is an unusual year because last year’s babies where protected from the virus due to lockdown and school closures.
As things have opened up again, they have been exposed to RSV, so more babies are presenting with bronchiolitis than usual for the time of year.
Our hospitals have already had admissions in June and July for a virus that usually circulates in the autumn.
The issue was discussed at a recent system-wide Winter Surge Planning Summit, which more than 40 people attended. We heard some of the ways that our paediatric services are managing the impact of the early surge, and we also discussed some possible solutions to help open more beds, care for children at home where possible, and to carry on with ‘business as usual’ while managing the additional pressures.
Following the summit, a paper was produced to alert providers and commissioners of services about the current situation and what may come, as well as those solutions that were discussed. The paper was well-received and as a result we will be taking forward some actions to ensure our children and young people receive the best and safest care as close to home as possible.
(Image above shows a social media graphic which forms part of Public Health England's information campaign about RSV).
Since 2015, there have been two networks in Greater Manchester overseeing service improvement of the local neuro-rehabilitation (NR) and stroke pathways.
These are the Greater Manchester Neuro-rehabilitation Network (NRN) and the Greater Manchester Integrated Stroke Delivery Network (ISDN).
Following agreement to move to a single provider model for inpatient NR services, the NRN changed its focus in 2020 so that it only now supports the community pathway.
Unfortunately, the pandemic has delayed transfer of acute services to the single provider model led by Salford Royal but this work will resume in the coming months.
Whilst the two networks have always worked closely together, they currently operate under separate governance arrangements and associated budgets. This can lead to duplication for stakeholders involved with both organisations as well as unnecessary complication in decision making and also inefficiencies in terms of cost.
As a result, the boards of both networks have recently approved the merger of the organisations into a single structure. The network team is currently consulting with stakeholders on some of the finer detail of the changes and has begun streamlining the way it works.
The move to a single network should bring great benefits to both the NR and stroke stakeholders each network currently works with, and help to achieve the over-arching aim of making services better for patients and their families or carers.
The memory of seeing Denmark footballer Christian Eriksen collapsing on the pitch at the European Championships this year will stay with many people for a long time.
Thankfully, urgent medical assistance arrived immediately, and cardiopulmonary resuscitation and defibrillation were performed on the field, which ultimately brought him back to life.
Every week in the UK, 12 people aged under 35 die from sudden cardiac arrest. And in the UK each year, 30,000 cardiac arrests happen outside of hospitals - all requiring emergency resuscitation, with just one in 10 people surviving.
The Cardiovascular Network is currently awaiting approval to work alongside the North West Ambulance Service on an ‘Out of Hospital Cardiac Arrest (OHCA)’ programme, which aims to give people a better chance of survival.
The aim of the project is to deliver a common, seamless pathway of care for those with OHCA, from resuscitation, through to the Cardiac Arrest Centres, reducing variation in care while improving the quality of service and outcomes.
It is hoped survival rates for patients who suffer an OHCA can be improved from 5.7% to 13%, saving 240 lives across Greater Manchester and Eastern Cheshire over three years.
|